World Leprosy Day: Up to half of leprosy affected people face mental health issues
ILEP releases interactive report on leprosy and stigma ahead of World Leprosy Day
ILEP is shining a light on the invisible scars of stigma ahead of this year’s World Leprosy Day–themed around ending the stigma and discrimination associated with leprosy–with the publication of a new interactive report.
The report reveals that up to 50% of people affected by leprosy will face mental health issues, such as depression or anxiety. (1) Depression is the most common mental health condition among persons affected by leprosy. There is also an increased risk of suicide among people living with the disease. (2)
Zero discrimination: ending the stigma of leprosy sets out the links between leprosy, negative social attitudes, gender inequality, myths, legal discrimination and mental health issues. The report argues that if we are to achieve zero leprosy, we must end the stigma and the laws and practices that discriminate against people affected by leprosy and their families.
The voices of women, men and children affected by leprosy are heard throughout the report. Rachna Kumari, member of the panel of women and men affected at the International Federation of Anti-Leprosy Associations (ILEP), and Community Mobilizer in the LEPRA Society in India, describes her experience:
“In India, humiliation and prejudice related to leprosy are very harsh, even more to a woman. My parents-in-law kicked me out of the house. My parents spent all their money supporting me and taking care of my children while I looked for medical assistance… Being affected by leprosy, especially if you are poor, is a heavy burden. There is no hope in the childhood and future of affected girls. Violence against women is threefold: gender, stigma and disabilities. It causes suicidal thoughts in women.”
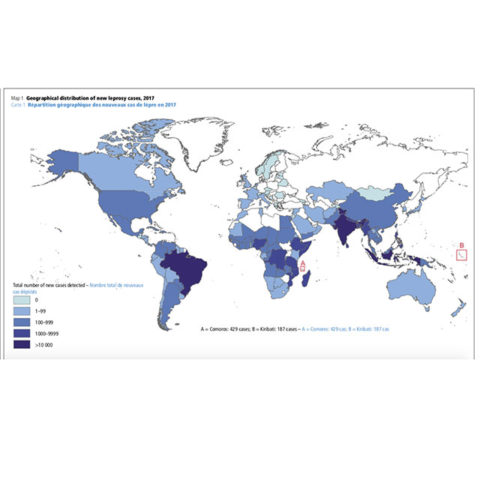
Every year, more than 200,000 persons are diagnosed with leprosy worldwide. While the disease is easily curable if detected early, around 6 million treated people affected by leprosy experience life-long disabilities or discrimination, or both.
Many live in some of the world’s poorest and most marginalized communities. Individuals affected by leprosy often experience rejection, shame and social exclusion from work or school.
These negative attitudes can also create a barrier to treatment, hindering efforts to stop the disease transmission at a global scale. Stigma, prejudice, and discrimination can prevent people with the symptoms of leprosy from seeking and accessing medical help, which delays diagnosis and treatment.
ILEP CEO Geoff Warne says: “We understand that achieving zero leprosy is not solely a medical issue. We need to change the way the disease is perceived and talked about within societies. This is no small task. But it is heartening to see the success of NGOs and organisations of people affected by leprosy who are demanding that the human rights of affected persons are upheld.
“I believe that this report, and World Leprosy Day later this month, will help to break down barriers, raise awareness and support the efforts of those fighting for social inclusion and mental wellbeing for everyone affected by leprosy.”
Ends
Notes to Editors
[1]Lepra publication “Building the case for the integration of Mental Health services in leprosy and lymphatic filariasis programmes” 2018 https://www.infontd.org/resource/building-case-integration-mental-health-services-leprosy-and-lymphatic-filariasis?aresult=0
[2]Gurvinder Pal Singh, Psychosocial aspects of Hansen’s Disease, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3505422/