Archives
World Health Summit
Leprosy Research Initiative Spring meeting
PEP4LEP 2.0 International Project Dissemination Meeting
2026 NNN Conference
World Health Assembly

Access delayed, rights denied
This year’s report to the UN General Assembly by the UN Special Rapporteur for leprosy, Beatriz Miranda Galarza, focuses on bottlenecks in the leprosy drug supply chain and their impact on affected persons. The Special Rapporteur’s starting point is that timely access to medicines and treatment is a fundamental human right. Since delays in leprosy medicines proportionately affect marginalized populations, and present greater risk of disability, this basic right is reinforced by the Convention on the Rights of Persons with Disabilities. This obligates States to ensure equality, including adequate healthcare, for persons with disabilities, including those affected by leprosy. How then to respond to what happened in Nigeria in 2024, when delays in MDT supply resulting from new domestic testing rules and bureaucratic delays affecting around 3,000 patients including 800 children?
Right to treatment
The Special Rapporteur makes the case that a human rights-based approach links access to medicines with broader State obligations to eliminate discrimination, marginalization and health inequities. She observes that WHO includes multidrug therapy for leprosy (MDT) on its Model List of Essential Medicines that require continuous availability. She then considers the issue from the perspective of international legal obligations and the CRPD and other global human rights conventions, and gives examples of courts in leprosy-endemic countries that have interpreted access to medicines as an enforceable human right.
Leprosy drug supply chain
The Special Rapporteur then examines the supply chain for MDT, remarking that this is especially important because, unlike many other drugs, MDT is not commercially available. Her report covers manufacturing and production, forecasting and procurement planning, donor coordination and international procurement, international shipping and customs clearance, and national warehousing and internal distribution. For each element, she provides specific examples of bottlenecks that have caused, or have potential to cause, delays preventing patients from getting the drugs they need. For readers interested in how the supply chain works and what can go wrong, this is instructive material.
Impacts on persons affected by leprosy
The Special Rapporteur describes the negative consequences of treatment delays caused by drug stock-outs. She describes impacts in terms of greater risk of nerve damage and disability. There is also mention of drugs to treat leprosy reactions, and the report comments that these drugs are poorly prioritized, excluded from essential medicine lists, and face regulatory, funding, storage and distribution challenges. The report also looks at other consequences. Anxiety, depression and suicidal ideation are common among persons facing uncertainty about treatment. There are also economic and livelihood effects. The report summarises this section pointing out, among other consequences, that non-supply of essential leprosy medicines amplifies the risk of the disease spreading to close contacts, and that increased physical impairments as a result of delayed treatment have lifelong impacts on the individual – as well as costs to the state health system.
Conclusion and recommendations
The Special Rapporteur summarises her conclusions at the end of the report, along with a set of recommendations to UN member states and other stakeholders. She reiterates that access to leprosy treatment is a human rights issue, and that in leprosy the drug supply chain is fragile and donor-dependent: bottlenecks exist at every stage and may cause cumulative delays which have life-altering consequences for patients and their families. Overall, she finds that States have limited ability to forecast, procure or track medicines independently. One result is erosion in public trust in the health system.
The recommendations are comprehensive. The first set of recommendations covers the elements of the supply chain: ensuring predictable and timely supply of leprosy medicine, strengthening forecasting and procurement systems, addressing regulatory and customs delays, and improving last-mile delivery and storage. There are also recommendations around involvement of persons affected by leprosy in supply chain monitoring, redress for persons suffering negative consequences from delayed treatment; and working towards greater national self-sufficiency and less reliance on aid.

Global leprosy (Hansen disease) update 2024: Beyond zero cases – what elimination of leprosy really means
ILEP Technical Commission commentary
The Global Leprosy Update for 2024 has been published by the WHO Global Leprosy Programme in the Weekly Epidemiological Review (WER) and updated in the Global Health Observatory. This much-awaited report has a mix of encouraging trends and a few issues of concern. The report applies the Leprosy Elimination Framework (LEF) published in 2023, to track progress.
It is encouraging to see 188 countries reporting in 2024 (an increasing trend), from all 6 WHO regions including all 23 of what WHO classifies as global priority countries for leprosy. However, a notable exception has been the United States of America which did not submit data despite consistently submitting data in previous years. This is an issue of concern since state-level reports indicate detection of new locally acquired cases in 2024. Globally, 172,717 new cases of leprosy were reported in 2024 including 9,397 children, 69,394 (40.2%) women and 9,157 (5.3%) with Grade 2 disability. Though new cases overall have decreased by 5.5% compared to 2023 (182,815), there are mixed trends in new case detection data among the global priority countries. Thirteen of the 23, including India, have shown a decrease while the remaining 10 have shown an increase of around 25% (e,g. the Philippines, Comoros and Sudan). It is a matter of concern that the 10-year trends for new case detection in some of the 23 global priority countries seem to be stagnant. The decreased number reported by India (approximately 7,000 cases) may be due to lack of activities (case detection campaigns). On the other hand, this decrease could be a true reflection of the leprosy situation in the country, as it is in line with decreasing numbers (new patients as well as the child rate) in the previous years. Perhaps this may be a positive development.
Unfortunately, the decrease in new case detection in South Sudan (by 60.2%), Somalia (by 34.2%) and Ethiopia (19.3%) is most likely due to worsening security affecting leprosy programmes.
Using a DHIS2-based software allows for more detailed and disaggregated data on leprosy cases to be reported to the WHO. New child cases reported were 9,157 which is a slight decrease from 2023 (10,322). An interesting metric is the disaggregated age-related data for 2,298 of these new child cases reported by 56 countries. 78.8% were aged 10-14 years, 22.6% aged 6-9 years and 4.6% aged <6 years. This implies that almost 25% of new child cases are under the age of 10 and need an adapted MDT regimen from the standard child pack which is supplied by the WHO for children aged 10-14. A matter of concern is the number of children with Grade 2 disability at the time of diagnosis – 289 (3.1%). This implies not only delayed diagnosis but also a new generation having to grow up with the burden of leprosy-related disability.
Encouragingly, 75 countries submitted data on leprosy reactions (14,689 cases with Type 1 reactions and 5,652 with ENL). This data most likely reflects the presence of reaction at the time of initial diagnosis, and the number is most likely much higher as a large percentage of persons diagnosed with leprosy develop reactions after starting MDT. Hopefully, this data will start to appear in future reports, especially for reactions that may have happened during the period on MDT. For the first time, nerve function assessments done at the completion of treatment were reported for almost 16% of new cases.
A major area of concern is that the active case finding data is very limited, with only 90 countries (including 20 global priority countries) providing data on contact screening (9,914 new cases detected through contact tracing). Of these, only 37 countries (including 9 global priority countries) provided data on PEP provision. The reasons for this are unclear, but may include some academic objections and, probably more importantly, significant inertia and logistic difficulties, as well as availability of rifampicin.
MDT, with its ability to quickly reduce infectiousness and limit disability, has to be taken regularly and completely to maximize and safeguard its impact. Out of the record 188 countries reporting this year, data on treatment completion rates for MB and PB were available for only 96 (representing ≈51%) and 81 (representing ≈43%) countries, respectively. Additionally, antimicrobial resistance (AMR) reports were received from only 23 countries. An issue of concern here is that India has not submitted AMR data for the past 3 years. Urgent deliberate actions are required to improve treatment and AMR surveillance and reporting as critical quality measures of leprosy control services.
Whilst surveillance is below standard recommendations, for countries with available data, treatment completion rates were highly variable and sub-optimal (<85%) in 9 countries for MB and 7 countries for PB, while a worrying total number of 4,365 individuals (3,850 diagnosed as MB and 515 diagnosed as PB) were lost to follow-up during the reporting year. Additionally, out of 2,109 cases tested for resistance, 27 cases were resistant to rifampicin (26 of these were re-treatment cases), 23 to dapsone (20 of these were re-treatment cases) and 4 re-treatment cases were resistant to both rifampicin and dapsone. Tailored interventions to support adherence to MDT are urgently needed.
The number of countries that reported adverse drug reactions in relation to MDT increased, with 32 countries reporting a total of 263 adverse drug reactions of which 235 were related to dapsone. Continuing to gather data on this issue will support the research for newer anti-leprosy drugs.
The report also highlights 81 discriminatory laws reported by countries. However, ILEP’s database shows 140 discriminatory laws. This difference in numbers is mainly because WHO’s report includes information directly reported by countries through DHIS2. Perhaps ILEP should coordinate with WHO to reflect the correct number of discriminatory laws in existence.
In summary, it is encouraging to see an increasing number of countries reporting leprosy data and a decreasing trend in the number of new cases detected, including a continuous gradual reduction in the child rate over the last 15 years. However, critical challenges also remain and need to be addressed. These include ongoing transmission, stagnant or increasing burden of new cases in some of the 23 priority countries, low participation from countries in AMR surveillance and increasing number of cases in island countries despite ongoing, active work. If the good progress achieved thus far is to be consolidated, more countries need to be encouraged to do active case finding through contact screening and PEP.
Of note, Jordan became the first country to be verified and acknowledged by WHO for the elimination of leprosy disease in 2024. The year 2025 marks 50 years of WHO’s partnership with the Nippon Foundation and 25 years of partnership with Novartis – this is the foundation for the global provision of MDT, so a definite cause for celebration.
The WHO report ends with an important message: “a person-centred approach must remain integral to all efforts!”
ILEP Technical Commission
October 2025
Pondicherry Municipalities act 1973, section 378
Madhya Pradesh Municipalities Act, 1961
IDDC General Assembly
ILEP Members’ Assembly
2nd International Conference on Tropical Dermatology

Roundtable on mental health, wellbeing and person-centred approaches
This Roundtable, hosted by Africa CDC in partnership with Anesvad Foundation, CBM Global and Liverpool School of Tropical Medicine, was held on 24 January in Kigali, Rwanda directly after the International Conference on NTD Research. Thank you to Maneesh Philip (from ILEP member Effect Hope) and other ILEP member colleagues for this report for ILEP Update readers.
Aim
The aim of the Roundtable was to enable progress in addressing the intersection of mental health and wellbeing, stigma and NTDs. These are key priority areas in the new Africa CDC NTD Strategy, the WHO NTD Roadmap 2021-2030 and other strategic frameworks. In particular, the Roundtable explored concrete actions to increase investment in mental health and NTDs across different sectors, and to strengthen efficient mechanisms for allocation of funds.
Background
The Roundtable was convened in a positive context. Research has demonstrated effective integration of mental health and wellbeing considerations into support services for people living with the effects of NTDs. There is a paradigm shift in global strategic frameworks towards person-centred approaches, consideration of mental wellbeing, and integration of services across sectors that impact on the lives of people affected. However, NTD services still tend to largely focus on preventive chemotherapy or on provision of limited medical services for people affected. Some countries are starting to work across vertical programmes, for example to improve access to mental health care for people with NTDs, or to coordinate access to social interventions like livelihoods with other sectors. Welcome developments are improved collaboration between government and non-state providers, and a stronger role for organisations of people affected by NTDs.
There is now well-established consensus on what changes need to be made, and an increasing technical capacity and political commitment to implementing these changes. But if the required structural reform is to be successful, domestic and external financing are required to support scale-up of good practice examples. At present, only a tiny proportion of funding for NTDs is directed to this area of work, despite being identified as a priority in the major consensus documents. The Roundtable brings collective expertise together to consider how resources can be effectively used to support global strategic shifts towards person-centred and community-driven approaches, while maintaining momentum in reducing prevalence of NTDs.
Key points from the Roundtable
Africa CDC shared its strategy for strengthening health systems across Africa, focusing on mental health, non-communicable diseases, infectious diseases, and NTDs. Key pillars of the strategy include integration, capacity building, collaboration, research, and resource mobilization. They have three flagship programs:
- Mentorship for NTD Program Manager Leadership
- Investment Case to build stronger evidence for funding
- Integration into primary healthcare and data systems (e.g., DHIS2).
Liverpool School of Tropical Medicine (Julian Eaton) emphasized the need for integrating mental health and NTDs, highlighting evidence that people with NTDs are more likely to experience mental health issues. He stressed the importance of funding and policy support for these integration efforts, with examples like the Global Fund’s commitment to ringfence funding for mental health.
Liberia (Karsor Kollie) discussed the challenges of integrating mental health into NTDs, citing the need for leadership, advocacy, evidence around economic benefits, and sustainable financing. Liberia shared an example of successful integration through the REDRESS project (mentioned above), which highlighted the need for policy changes and resource mobilization which are now being implemented through the TRANSFORM project (integrated NTD program).
Nigeria (Gabriel Afolayan) focused on starting integration at the policy level, using the NTD Master Plan as a framework. He highlighted the need for coordination across sectors, clear strategies, tailored interventions, and training for health workers.
Anesvad Foundation (Inés Egino) has focused on a person-centered approach to skin NTDs in West Africa, integrating mental health with health systems strengthening. Anesvad’s strategy emphasizes community-based approaches, government support, capacity building, and collaboration.
END Fund suggested including mental health indicators in NTD dossiers and advocated for integrating mental health into national health sector plans.
Effect Hope (Maneesh Phillip) has supported Liberia’s NTD program since 2012 by developing an integrated approach to health systems strengthening, starting at the national policy level and extending to county, primary healthcare (PHC), and community levels. This effort evolved through various phases, now under the TRANSFORM project, which supports Liberia’s NTD Master Plans from 2016-2020 (extended to 2022) and the new Master Plan for 2023-2027. Effect Hope collaborates with partners like Anesvad Foundation and American Leprosy Missions, ensuring sustained funding for these initiatives. As part of the REDRESS project, mental health was incorporated into the new Master Plan and is included in TRANSFORM’s implementation, with a focus on training health workers at all levels. Effect Hope also partners on similar projects in other countries in Africa and Asia, studying models that improve access to care for people affected by NTDs.
Outputs and next steps
The Roundtable revealed a shared commitment to integrating mental health into NTD programs across various African countries, with emphasis on leadership, policy changes, evidence-based approaches, and sustainable funding.
The organizers will publish a report of conclusions from the Roundtable, for sharing with participants’ organisations and to encourage further engagement to raise the profile of person-centred approaches and investment in sectoral reform. The report will also be shared with key organisations such as WHO, UNECA and other UN agencies, African Union, World Bank, African Development Bank, WAHO, ECOWAS and other African regional economic blocks.

International Conference on NTD Research
This month, COR-NTD and the African Research Network for Neglected Tropical Diseases (ARNTD) hosted the second International Conference on NTD Research (InCORNTD) in Kigali, Rwanda in collaboration with the Ministry of Health. Over 500 researchers, academics, and policymakers met during the three-day conference aimed at bridging the gap between research and implementation, ensuring that knowledge translates into tangible impact in the fight against neglected tropical diseases (NTDs). You can watch highlights on the COR-NTD website and full recordings will be made available later. Thank you to Liesbeth Mieras (from ILEP member NLR) and other ILEP member colleagues for this day-by-day report on topics particularly relevant to ILEP Update readers.
Day One: 20 January
Opening remarks
There were welcomes by Pat Lammie (Director of COR-NTD), who emphasized catalysing new collaboration during the conference, and John Amuasi (Executive Director of ARNTD), who motivated participants to come up with bold ideas to put research into action to tackle NTDs.
Noella Bigirminana, Deputy Director General of the Rwanda Biomedical Centre, emphasized Rwanda’s commitment to eliminating at least four NTDs as a public health problem by 2030. She highlighted the importance of multi-sectoral collaboration and establishing essential services to achieve this ambitious goal, and overcoming the inequity related to NTDs. ‘Rwanda is committed to increasing domestic resources allocated to NTD control interventions. Investing in research is critical for generating evidence-based strategies. I call for strengthened multi-sectoral collaboration through the One Health Approach, which will not only contribute to eliminating NTDs but also help achieve the WHO NTD Roadmap targets, the Sustainable Development Goals, and other continental and global strategic objectives’.
Dr. Mosoka Papa Fallah, Deputy Director of the Africa CDC, underscored the timeliness of the conference, calling for leveraging cutting-edge technology to accelerate the elimination of NTDs. ‘We are in an era of groundbreaking scientific discoveries, from the rapid development of the COVID-19 vaccine in just 12 months to advancements like the recent discovery by Japanese scientists of pathways to regenerate teeth at any age. Yet, despite these incredible achievements, 1.2 billion people in Africa and parts of Asia suffer daily from Neglected Tropical Diseases” Dr Mosoka posed two thought-provoking questions to all concerned actors:
- Does poverty serve as an invisible magnet that attracts NTDs?
- Do NTDs persist among the poor because they are poor, disempowered, and faceless?
Through these questions he invited deeper reflection on the structural injustices, weak health systems and societal dynamics that perpetuate the burden of NTDs, including the mental health consequences.
Morning presentations
- Health systems integration for schistosomiasis and other NTDs. Presentations focused on integrated ways to implement Mass Drug Administration (MDA) campaigns targeting children, such as MDA combined with mother and child health, including vitamin A distribution.
- WHO research and development blueprint. This was mentioned in the October Update where we encouraged readers to sign up to participate, to maximise the number of voices contributing. The deadline has been extended. One of the driving issues is that progress towards the 2030 NTD goals is too slow, and this is related to the fact that there is relatively limited research on NTDs, compared to for example malaria. Questions posed by speaker Anthony Solomon included: Are we doing enough? Do we coordinate and collaborate enough? Are we addressing the right questions?
- Post-validation surveillance. Abdel Direny shared PATH’s Landscaping report: Integrated surveillance planning toolkit for NTDs in post–validation or verification settings
- iCHORDS encouraged participants to join its Community of Practice which aims to mobilize social and behavioural science into practices that meet the needs of NTD program implementers and partners, to reach the WHO 2030 NTD Roadmap targets. Services include podcasts, knowledge exchange cafes, a mentorship program, quarterly newsletters, blog posts and focus area support.
Visceral Leishmaniasis (VL)
20 million people are at risk of contracting VL; 95% of patients will die if not treated. Targeted vector control (sandflies) is lacking and new breeding sites are emerging. More positively, Bangladesh has achieved elimination of VL as a public health problem, so the challenge is how this can be achieved in East Africa. The solutions to ongoing transmission lie in innovative interdisciplinary control approaches, covering:
- Early diagnosis and treatment
- Integrated vector management
- Effective disease surveillance
- Advocacy, social mobilisation and partnership
- Research and development
Contributors to the session included DNDi – Best science for the most neglected which works with partners in low-and middle-income countries to develop treatments for various diseases. These include their Leishmaniasis East Africa Platform (LEAP). WHO has launched a new strategic framework to eliminate VL in East Africa.
The challenges for VL elimination are very similar to the challenges for leprosy control: early detection, early treatment, care, preventive measures, point of care diagnosis, training, awareness, logistics (medication), surveillance, poverty reduction. Diagnosis, treatment and care for people with skin NTDs is a pathway to stronger health systems.
The session identified these requirements for effective surveillance:
- Systematic collection and analysis of data to monitor disease and inform public action
- Improve by digitization, training etc
- Detect outbreaks
- Monitor trends
- Promote equitable access
- Develop policies for prevention, control and elimination
- Identify new foci (eg consequences of climate change)
Day 2: 21 January
Shape the future for Skin NTD diagnosis – successes and operational challenges
This session was chaired by Kingsley Asiedu (WHO NTDs) and moderated by Liesbeth Mieras (NLR). Rapporteur was Suzan Trienekens (LRI). The full report and slides will be made available in a subsequent ILEP Update.
Sharing and developing practical tools for the integration of NTDs and mental health.
Julian Eaton, CBM Global, talked about the essential care package that is under development by the NNN DMDI (Disease Management, Disability and Inclusion) group. He stressed that treatment and care should aim to not interrupt the income of the patient and to support the patient in their daily life to the extent possible. Research priorities included prevalence and risk factors, and development and evaluation of integrated interventions.
This session continued in a subsequent side meeting. Interventions that were highlighted included:
- Better Mental Health for People with NTDs in Nigeria | Anesvad
- Strengthening people-centred health systems for people affected by severe stigmatising skin diseases in Liberia – REDRESS Liberia (see next section below)
- Guide on Basic Psychological Support for Persons Affected by Neglected Tropical Diseases (BPS-N) | NLR and InfoNTD
- The Livex project of RedAid Nigeria: LIVEX – Empowering Lives: A Landmark Dissemination Meeting on Improving Physical and Mental Wellbeing of Persons Affected by NTDs
- The ILEP-NNN Stigma Guides. Guides on Stigma and Mental Wellbeing | InfoNTD
Follow-up steps were agreed, aimed at making tools easily available and accessible, as well as flexible to enable contextualisation. An online workshop will be organized to get a bigger group together to further discuss: What is good about existing materials? What is missing? What is the best/preferred format so that tools are accessible and useable by health systems?
REDRESS
REDRESS, profiled in the August 2024 Update, is a comprehensive project in Liberia focused on severely stigmatizing skin diseases including leprosy. The very comprehensive combined REDRESS manual was presented by Rosalind McCollum (Liverpool School of Tropical Medicine) and Emerson Rogers (MOH Liberia). The manual includes not only training materials, but also pre-and post-tests and reporting tools. There is an all-condition algorithm (page 112) which is useful as a wall-chart for mid-level Health Workers. It is Liberia-specific in terms of diseases included, but it can be adapted to other contexts as well. There are multiple tools embedded in the manual as annexes, for example the Basic Psychological Support for person affected by NTDs (BPS-N), a diagnostic communication job aid, and mental health indicators within NTD case management.
Day 3: 22 January
Building sustainable financing for NTD programs: tools, challenges and collaborative solutions
The Task Force for Global Health has been working on Pathways to Sustainable NTD Elimination with the aim to empower and equip stakeholders with the tools and strategies needed to sustain the progress made in the elimination and prevention of NTDs, especially Onchocerciasis and Lymphatic Filariasis. By investing in the capabilities of national program managers, this initiative enhances advocacy efforts, bolsters the effectiveness of NTD programs, and positively impacts broader communities.
The tool can be downloaded at the link above in English and French, and Spanish and Portuguese versions will become available. There is an e-course consisting of 5 modules that you can access online. The tool helps to identify actors, including those who would normally not be thought of, to mobilize domestic resources and support the NTD programme, and to identify challenges and opportunities. Experience in Togo showed that the tool enables a full understanding of the messages that need to be drafted, and it can help engaging stakeholders. MoUs with MoH for medication supply and in-country distribution is another example. The tool also helps to understand how to present the return on investment.

NNN Conference 2024
The annual conference of the Neglected Tropical Disease NGO Network (NNN) has just finished in Kuala Lumpur, Malaysia. Once again, there was strong representation from the leprosy world including from ILEP members, seven of which contributed to sponsorship of the event. Around a quarter of attendees had connections with leprosy organisations, and most of them participated in a three-hour leprosy group meeting. A related highlight was the participation of persons affected by leprosy, LF and Buruli ulcer. Indeed, participation by affected persons, especially in research activities, was a theme featured in several conference sessions.
Leprosy group meeting
More than 50 participants joined the two 90-minute sessions of the leprosy group meeting. This year’s meeting covered three topics, only one of which was strictly leprosy. Wim van Brakel (chair of the ILEP Technical Commission) presented the WHO Leprosy Elimination Framework with a particular focus on the practical use of the Leprosy Elimination Monitoring Tool. Constanze Vettel (from ILEP member German Leprosy Relief Association) promoted the use of the NTD Inclusion Score Card (NISC) with particular reference to the impact of the use of this tool globally within GLRA. The second 90-minute session, led by ILEP CEO Geoff Warne, focused on identifying and overcoming the obstacles to the participation of persons affected by NTDs in research, especially operational research.
Anil Fastenau (GLRA) and Inés Egino (Anesvad) also led a one-hour special plenary session on the topic of participation in research, featuring the testimony of persons affected by NTDs from Sierra Leone, Nigeria and Liberia.
Sponsorship
ILEP was once again a Platinum sponsor of the NNN Conference thanks to financial contributions by The Leprosy Mission, NLR, GLRA, Lepra, SLC, FAIRMED and Fontilles. Associated with our sponsorship was a movie night in which ILEP members were well represented with some excellent short films.
Sungai Buloh
The ILEP Secretariat took the opportunity to organize a group visit to the Sungai Buloh leprosarium, on the outskirts of Kuala Lumpur. At its peak in the 1930s, this was home to more than 2200 men, women and children suffering from leprosy, and 80 mostly very old ex-patients still live there today. ILEP member Sasakawa Health Foundation has enabled the construction of a well-designed museum that shows the history of this place, and is advocating for its recognition as a UNESCO Heritage Site.
NNN’s future
The NNN Executive Committee has agreed on the need for a comprehensive review of NNN’s work, effectiveness, structure, operating model and sustainability. The outline and purpose of this review were described at an NNN members’ lunch meeting. The review is expected to run till mid-2025.

Global leprosy (Hansen disease) update 2023: Elimination of leprosy disease is possible – Time to act!
Commentary: Dr Paul Saunderson
The WHO Global Leprosy Programme has published the Global Leprosy Update for 2023, available on the WHO website. The report focuses on the new Leprosy Elimination Framework, published during 2023. The Framework consists of three distinct phases, which are easily described and understood, and appear to be scientifically robust. As long as the data are available, it is not difficult to see where any particular area (be it a country or a sub-national region), sits in the Elimination Framework. This Framework makes it easy to target our activities, so it is indeed time to act!
The first phase ends when the transmission of M leprae in that area has ceased – now defined as having registered no child cases of leprosy (under 15 years of age) for at least five years. An Excel-based tool, known as the Leprosy Elimination Monitoring Tool (LEMT), allows data to be recorded for each sub-national area (for example, each district), each year. The LEMT automatically classifies the concerned areas into the appropriate, colour-coded elimination phases according to the Leprosy Elimination Framework. It thus displays progress towards the elimination targets over time, for each district, and in aggregate, for the country as a whole.
One of the numbers in the report that struck me as particularly significant was that of 184 countries reporting, 110 reported zero child cases (see p 505 of the report), and according to the tabulated data, another 38 countries reported fewer than 10 child cases. This suggests that 148/184 (80%) of countries that reported are making good progress towards the end of this first phase of leprosy elimination. Every country and every sub-national area is different and on a different trajectory, but once data-points are plotted over a number of years, any progress can be seen, and areas with slower progress can be identified and assisted.
A second number (on page 508) was much more worrying. It is stated that of the 182,815 new leprosy cases reported, only 14,908 (8%) were detected through active case finding. Clearly this is not necessarily a very accurate figure, as some programs do not report it, but it may help to remind us that active case-finding (at present contact examination is the favoured method, and skin camps have proven very effective in many communities in Africa) is the key activity in any effort to ‘end leprosy’. It is also a common finding that when active case-finding is done rigorously in any particular endemic area, the number of new cases identified is usually higher than expected, suggesting a significant under-reporting of new cases globally. If post-exposure prophylaxis (PEP) is to be given, as recommended by WHO, it is easily carried out in the context of contact examination or a skin camp. It is unfortunate that the WHO update does not yet include more detailed statistics of active case finding and of PEP administration, as these are currently optional reporting fields.
Even people who do not favour PEP usually emphasize active case finding, which can be very successful over time, if carried out rigorously (for example, the decades long programme in Malawi reported by Prof Paul Fine and colleagues1). Another important reason to emphasize contact examination is that, by identifying new cases early, a significant decrease in disability can be achieved.
In summary, the good news is that many countries and many sub-national regions are making good progress towards zero leprosy. The main challenge, however, is to greatly expand active case-finding – particularly through contact tracing – in the remaining endemic areas, especially in the 23 WHO priority countries. This is a time-consuming and costly exercise, but it can be made much more efficient by carefully targeting hotspot areas. These can be identified by various mapping techniques and the LEMT is one of the best tools available, with its own built in mapping function (in preparation). While the new WHO paradigm gives us a framework for action, active case finding should be the main focus of our activities, ideally supplemented with PEP.
—-
1 LEP – KPS Team; The epidemiology of leprosy in Karonga District, northern Malawi 1973–2023: An analysis of leprosy’s distribution, risk factors, control and decline in rural Africa; Leprosy Review. 2024; 95; 1; 7-84; DOI: 10.47276/lr.95.1.7
US 8 USCS § 1285
Employment on passenger vessels of aliens afflicted with certain disabilities, including leprosy, is prohibited.
Virgin Islands 19 V.I.C. § 79
Persons affected by leprosy, and contacts, who fail to submit to necessary examinations will be fined (up to 100 USD) or imprisoned (up to 180 days) or both.
VI 19 V.I.C. § 77
All known contacts with a person afflicted with Hansen’s disease, including all family connections, by blood or marriage and all persons known to have Hansen’s disease, resident in the Virgin Islands, shall submit to examinations by the Commissioner of Health or by a physician licensed to practice in the Virgin Islands at intervals not to exceed 12 months during the first 10 years following the last contact and thereafter at the discretion of the Commissioner of Health.
Federal Law Number 28 of 2005 (Article 112)
If one of the parties has leprosy, obstruction of genital canals, or insanity before or during the marriage, the spouse could ask for the marriage’s rescission.
Midwives Registration Ordinance (Cap. 162)
The regulatory authority of midwives having the discretion to prohibit registered midwives suffering from any such scheduled infectious disease from attending women in childbirth.
Nurses (Registration and Disciplinary Procedure) Regulations (Cap. 164A)
Medical certificate required for a nurse to certify that she is not suffering from any such disease (as part of her application to register)
Swimming Pools Regulation
Persons affected by communicable diseases, including leprosy, are denied access to private (Cap. 123CA) and public (Cap. 132BR) swimming pools.
Commercial Bathhouses Regulation (Cap. 132I)
Persons affected by communicable diseases, including leprosy, are denied access to commercial bathhouses.
Prevention and Control of Disease Ordinance (Cap. 599)
Leprosy is expressly defined as a “Scheduled Infectious Disease” in HK’s main public health legislation. This definition includes diseases such as COVID-19, Anthrax, Chickenpox and Cholera.
GCA 10
Sections 3309-3321; 3328; and 3333 allow for several forms of discrimination on the basis of leprosy. These include requirement to isolate; police enforcement of isolation; destruction of property; closure of schools; specific disposal of corpses; restrictions to enter country.
Environmental Health Services Regulations, 2003
Compulsory segregation of people affected by leprosy (lists leprosy as a First Schedule disease).
Meat Industries Act 1996 (NT) s 42; Meat Industries Regulations 1997 (NT) r 64, sch 3
Persons who have reason to believe they are infected with or affected by leprosy must not enter or remain at an establishment from which meat for human consumption is dispatched; a holder of a licence permitting the dispatch of meat for human consumption who has reason to believe a person is infected with or affected by leprosy, must not permit that person to enter or remain at an establishment operated under that licence.
Migration Act 1958 (Cth)
Requirement of persons with leprosy to provide a health undertaking in order to obtain visa; undertaking requirements include reporting to the health clinic to which they are referred, placing themselves under the health clinic’s professional supervision, and undergoing any required course of treatment or investigation.
UN Special Rapporteur’s vision
In June, Beatriz Miranda Galarza, the UN Special Rapporteur on the elimination of discrimination against persons affected by leprosy (Hansen’s disease) and their family members, presented her first report to the UN Human Rights Council. The report describes the impact of the mandate since its establishment in 2017, her vision and priorities for the coming years, and her intended method of work. The report was informed by extensive consultation with persons affected by leprosy, as well as other stakeholders including ILEP.
Background: four approaches
The report begins with a description of the historical struggle of people affected by leprosy, from exclusion to recognition as holders of rights. The four approaches are the religious and moral approach, the scientific and administrative approach, the representative and cultural approach, and the human rights-based approach. The Special Rapporteur points out that these approaches may co-exist and that each has a positive contribution to make (as well as some negative implications).
Voice of persons affected by leprosy and their organizations
Consultations by the Special Rapporteur revealed positive effects, especially at the international level, since the mandate was created in 2017. At the local level, there are also positive effects. For example, some grass-roots organizations are more aware of violations of the rights of persons affected by leprosy in their own communities. For some organizations of persons affected by leprosy there is greater recognition than before, due to participation in human rights events related to leprosy and engagement with the United Nations. This effect was especially striking in countries where the Special Rapporteur had made country visits.
Key priorities for the mandate
Following consultation, the Special Rapporteur has selected five main priority areas for the next three years.
- Rights-based systems surrounding support and care for leprosy within the family and communal context, guided by reliable data regarding the mental, social and economic impact of leprosy on affected persons and their families.
- Intersectional issues and marginalized groups, with a focus on the challenges that persons with leprosy-related disabilities face in their daily lives, and particular reference to the circumstances of children, women, young people and older persons.
- Social, political and cultural considerations. These include the strengthening of social movements and activism, tackling the difficulties experienced by organizations of persons affected by leprosy, the preservation of leprosy history, living conditions in leprosy colonies or settlements, and migration factors in leprosy.
- Legal and economic dimensions – action on discriminatory laws, poverty and the need for socioeconomic empowerment.
- Environmental and conflict-related considerations, including factors such the effects of conflicts in worsening the already precarious living conditions of leprosy-affected communities, and the effects of climate change.
The first of these priorities will be the theme of the Special Rapporteur’s 2024 report to the UN General Assembly. Others on the list will no doubt emerge as themes for subsequent reports.
Guiding principles for the mandate
The Special Rapporteur has expressed three main principles that will support her mandate. They are:
- An ethics of care as a fundamental aspect of human life, challenging the sometimes negative attitudes around care and support.
- Contribution to a culture of listening to persons affected by leprosy. ‘The right of persons affected by leprosy to participate at every level of public and private life will not be realized unless listening is embraced as a practice that evolves into a culture.’
- Promoting cooperation and the co-production of policies and strategies, not only to support the mandate but to realize the goals of the leprosy rights movement as a whole.
To quote from the conclusion of her report, the Special Rapporteur ‘will promote a human rights approach guided by an ethics of care that places people’s voices at the centre and as the primary source of evidence, thereby contributing to the construction of a culture of listening and more equitable and just societies. The Special Rapporteur underlines the particularity of leprosy (Hansen’s disease) as a catalyst of social, political and cultural change, serving as a beacon for a more democratic, humane and diversity-respecting world. In the present report, she underscores the significant transformation for individuals affected by leprosy, as well as their families, organizations and allies, brought about by the implementation of the mandate.’

CRPD Conference of State Parties
ILEP member The Leprosy Mission (TLM) attended the United Nations’ 17th Conference of State Parties (COSP) to the Convention on the Rights of Persons with Disability (CRPD) this month. The COSP presents an opportunity to speak about the rights of persons affected by leprosy, usually as the only voice for the disabling effects of leprosy and NTDs.
Side event
TLM hosted a side event on the rights of persons with disability to work, partnering with the Government of Malta and others. The meeting room was full, but the UNTV recording of the event is here. The panel included OPDs, UN entities, the World Bank, and academia, with a keynote address by Ms Heba Hegrass, UN Special Rapporteur on the Rights of Persons with Disability.
Speeches at the conference
Two persons with lived experience of leprosy spoke at the conference. Amar Timalsina spoke during the Civil Society Forum on the right to work, with a particular focus on best practice. Mathias Duck made a speech during the general debate, asking delegates to remember leprosy and persons affected by leprosy through their work.
Progress on discriminatory laws
One of the founding principles of the CRPD is that there will be no discrimination in law against persons with disabilities. This makes the COSP an ideal space to talk to countries about laws that discriminate against persons affected by leprosy. At the last COSP, TLM started dialogue with Malta about an outdated discriminatory law which is now on the verge of repeal. Malta has offered support in speaking to the other nine Commonwealth nations with discriminatory laws. This year TLM started conversations with Australia about repealing two recently discovered discriminatory laws, and either continued or initiated linkages with UAE, Egypt, and Barbados which confirmed that a previous discriminatory law has been repealed.
CRPD Committee
The CRPD Committee is the body who is responsible for holding states accountable for their actions to implement the CRPD. The COSP elected new Committee members from Dominican Republic, the EU, Japan, Jamaica, Nigeria, and Uruguay. These individuals are in a position to draw the Committee’s attention to the rights of persons affected by leprosy, so they are valuable contacts.
Meeting with OPDs
The voices of persons affected by leprosy can be stronger when they are a part of the wider voice of the disability movement. When states seek to consult with Organisations of Persons with Disability (OPDs), for example, it is important that organisations of persons affected by leprosy are included. TLM built on the dialogue at the ILEP-hosted webinar on people’s organizations, which took place in January, by speaking to several OPDs that attended COSP17 to find out how organizations of people affected by leprosy can engage with these wider networks to have their voices heard.
Global Disability Summit 2025
Next year, the Global Disability Summit will be hosted in Berlin in April. At COSP17, the Summit hosts (Germany, Jordan and the International Disability Alliance) launched the commitment portal for the Summit and called on states, NGOs, funders and others to make measurable, impactful commitments related to the CRPD and SDGs. This year the portal allows for commitments in partnership with others, so ILEP members can make joint commitments or partner with other actors.
In the words of the organisers, ‘the process of developing the commitments is as important as the commitment itself’. IDDC offers briefing sessions on the Summit on 24 July and 25 September.
World Summit for Social Development 2025
This summit, scheduled for 2025, follows the major Summit for the Future in September, and is being pitched as an opportunity to reduce inequalities and to promote social justice, inclusion, equity and non-discrimination.
Any questions on COSP17 of the above developments can be directed to Mathias Duck and Tim Burton.
77th World Health Assembly
The ILEP Secretariat was in Geneva during the seventy-seventh World Health Assembly, held in the last week of May. The Assembly is the peak event for WHO each year. Big-picture outcomes this year were the adoption of WHO’s strategy or plan of work for 2025 to 2028, a resolution on climate change and health, and a resolution on social participation with a particular focus on promoting the voices of people in marginalized situations. But in addition to the main meetings there is a wide array of side events and opportunities for linkages and networking.
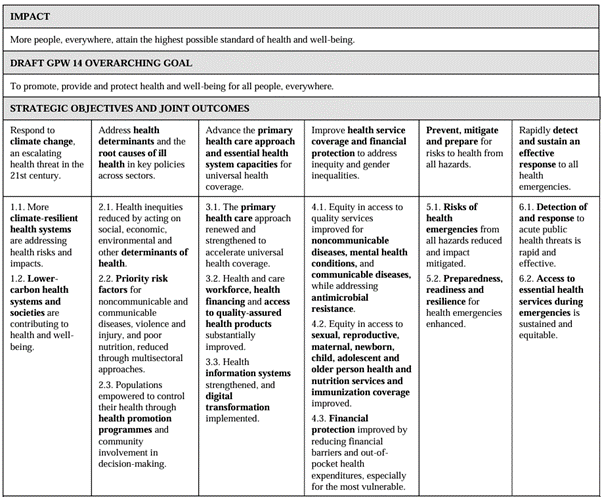
WHO Plan of Work 2025-2028
The Plan of Work – which is summarised in the table below – is important to ILEP and its members. Partly that is because organizations in official relations with WHO – like ILEP – are expected to develop and report on three-year cooperation agreements that need to link with the Plan of Work. But also, as ILEP members interact with WHO both globally and at country level, it is relevant to be able to refer to those elements of the Plan of Work that ILEP members are working collaboratively towards. The second objective (social determinants), third objective (health systems, including data) and fourth objective (especially equity of access to health services) seem particularly relevant. See here for the Director-General’s report that contains the 2025-2028 Plan of Work.
Climate change and health
In passing this resolution, Member States built on previous decisions that recognised the inter-relationship of climate change and health. The resolution points out that the pace and scope of mitigation and adaptation efforts are being surpassed by climate change threats, and that any further delay in concerted global action will miss a brief and rapidly closing window of opportunity to secure the goals of health and wellbeing for all. It also points out that climate change is worsening existing health inequalities and that people in marginalized and vulnerable situations can be most at risk of negative climate change impacts. The commitments agreed by Member States are arguably not as strong as the identified risks, but there is agreement to strengthen the implementation of WHO’s global strategy on health, environment and climate change, without diverting resources meant for primary health care. Members interested in ongoing advocacy on the effects of climate change may find it relevant to look more closely at the resolution and also at the forthcoming global plan of action on climate change.
Social participation for universal health coverage, health and well-being
WHO defines social participation as empowering people, communities and civil society through inclusive participation in decision-making processes that affect health. This resolution repeated previous agreements about the need to promote participation of people in vulnerable and/or marginalized situations including persons with disabilities and those who are furthest behind. The resolution urges Member States to implement, strengthen and sustain regular and meaningful social participation in health-related decisions. The relevance for ILEP members working with people affected by leprosy is obvious. We recommend close study of the resolution especially by ILEP members that are working to empower organizations that represent persons affected by leprosy in interaction with central and local governments.
Skin Diseases as a Global Public Health Priority
This well-attended side event was hosted by the International League of Dermatological Societies (ILDS) and GlobalSkin, an international alliance of patients of skin diseases. Presenters showed that skin diseases stand in seventh place in terms of YLDs (years of healthy life lost to disability and illness) and affect 5% of the global population at any given time. Perhaps less surprising was the comment that data quality is a major issue across most skin diseases – not just skin NTDs. Follow-up actions by the ILEP Secretariat will include:
- Reconnection with GlobalSkin to advocate for inclusion of organisations of persons affected by leprosy and other skin NTDs in their networks. We previously discussed with GlobalSkin the limitations of the word ‘patients’ in their name and we will continue to develop that theme.
- Further discussion with Dr Kingsley Asiedu (WHO) around a comment in his speech urging ILEP to be more involved in the general skin diseases community.
- Response to a planned WHA resolution on skin diseases, proposed by ILDS, GlobalSkin and other stakeholders. The plan is to bring a resolution for the consideration of the WHO Executive Board in January 2025, calling for investment to expand expertise in skin diseases especially at PHC level; to expand research capacity to provide innovative diagnostic tools and new treatments for skin diseases; and to strengthen global skin health databases to inform planning needs and monitor progress.

COR-NTD funding opportunities
COR-NTD is the Coalition for Operational Research on NTDs, one of the programs of the Task Force for Global Health. This year COR-NTD has decided to host regional events instead of its usual large annual event in the USA. The first of these, in April 2024, was in Delhi, co-hosted by the WHO South East Asia region. There are plans for events in the WHO Western Pacific region in September and the WHO Africa region possibly in December.
Integrated surveillance
The main theme of the Delhi meeting was opportunities for integrated NTD surveillance, specifically including leprosy, both before and after interruption of transmission has been verified. Several presenters commented that in the South East Asia region there are several disease surveillance processes, including in TB, malaria and other vector-borne diseases. The idea is not to take a prescriptive approach but to find sustainable surveillance models into which leprosy and other skin NTDs can be integrated. The benefits of integrated surveillance seem clear: it is effective in reaching multiple diseases, it is efficient in terms of time and money, and it is better for community members because of attention to multiple diseases at the same time. But presenters also highlighted various challenges to integrated surveillance: the additional logistical work required; the need for a ‘win’ for all the diseases involved; financial constraints and the need to build agreement with multiple donors; the need for the selected approach to be sustainable over several years; and the reality that NTDs may need to compromise their expectations in order to gain access to existing surveillance programs.
COR-NTD funding
Although COR-NTD’s main priorities have been diseases other than leprosy, Pat Lammie (COR-NTD President) said that he expects leprosy to be more of a focus in 2024 and beyond. Partly this reflects an ongoing trend in the approach of the United States Agency for International Development (USAID). COR-NTD has been awarded a new cooperative agreement with USAID entitled Ending Neglected Diseases through the Operational Research Program. To illustrate, Dr Lammie commented on USAID’s offer of funds to WHO regional offices to come up with new initiatives across any of the NTDs; on USAID’s increasing interest in skin NTDs; and on the availability of funding for diagnostics and morbidity management, both highly relevant for leprosy.
Operational research into integrated surveillance
Pat Lammie and other senior COR-NTD personnel made it clear that research into how leprosy and other NTDs can be integrated into existing surveillance systems is a fruitful topic for their operational research funding. The preference is for multi-country studies, though COR-NTD would consider a clear justification for why a country’s uniqueness may lead to the need for single-country research. Research also needs to be actionable, or solution oriented. For example, COR-NTD would like to see operational research that tests the efficacy of different NTD integration approaches in different settings.
We recommend that Members continue to check the COR-NTD website for any upcoming calls for open solicitations: https://www.cor-ntd.org/funding-opportunities.
Submission on human rights of persons affected by leprosy in Pakistan
ILEP coordinated a submission to the 19th Pre-session of the CRPD Committee recommending inclusion in the List of Issues of a set of measures assuring the human rights of persons with disabilities, including persons affected by leprosy, in Pakistan, especially regarding the plight of older people and the leprosy villages.

Nsimbu, 60, Kuakua
Nsimbu lives with his wife. They have 6 children, all of whom are grown up and living elsewhere. He’s a farmer and been educated to class 2.
“Five years ago I started to get wounds on my legs. I was also getting feverish around this time, though I thought that was due to malaria. I had patches covering my body.” His wife agrees with him: “In those two years I saw so many wounds, and he always had a fever.”
“I couldn’t work hard in this time, I couldn’t work fast. My wife was doing everything. The fever incapacitated me constantly.”
It was his wife who eventually told Mathos at the TLM apprentices’ workshop, and he referred him to hospital. He was diagnosed three years ago with leprosy.
“When I was diagnosed I was depressed and distraught. I was ready to drink battery acid and end my life. But the doctors told me I’d be ok and gave me hope, and that’s why I’m alive.”
“When I’d completed the MDT, I observed changes in my legs. Mathos provided me with bandages (from TLM), and gave me self-care training. I still do self-care every morning and evening.”
Nsimbu still has anaesthia on his feet and legs, though at first says he has full sensation. He clearly doesn’t, but some sensation has come back.
“I still get tired doing farm work. But I’m happy now. I accept how I am, because I’ve received a lot of advice from doctors and community leaders. Life is still hard, but I have no worries.”
“I’m very grateful to Father Placide and TLM Congo. Without them I wouldn’t be alive.”
Nsimbu has received some money for welfare. He’s used it to buy food, as well as pay some people to farm his land when he’s unable.
Thank you to TLM for contributing this story for #WorldLeprosyDay!

Remy , 24. Leprosy Settlement, Kongo Central
Remy lives in a small leprosy settlement of just a few houses, built by the government in the 1980s for those affected by leprosy. It is not too far from an old hospital in the forest outside of a village, and the settlement was intended for those that needed to stay short term while taking MDT.
Families now live here permanently, and TLM has since built a well here, and helps with wound dressings etc. Remy was born here.
He lives with his parents and two siblings. There are 7 brothers and sisters in total, though 4 live away from home. He’s the second youngest. His father, Fabien (also pictured), 70 was also affected by leprosy.
He’s finished high school, and does various jobs at home – farming cassava, palm oil, and honey. Beekeeping was introduced in this small village in 2011 by TLM, and they are known for selling honey. “I have qualifications, but to start off jobs you need money to pay bribes.”
Remy has done technical studies in electronics, but wasn’t able to touch things in the workshop because of weakness in his hands. It was in 2013 that he got the first symptoms, while studying at secondary school.
Since his family were very familiar with leprosy, he was taken straight to the local hospital and diagnosed. “As I was born here, I know the disadvantage of leprosy, and I lost hope. I thought with this, I’ll lose sensitivity and not be able to do anything with my life. I was fearful that it would eventually kill me.” He no longer thinks like this about leprosy, having been educated better.
“At school none of my classmates would sit near me. I was studying in the nearby town of Nsioni, and it was difficult for me to continue going to school at this time.”
“When I started taking MDT my urine became red, and my skin went darker and dried up. But after two months my hands became strong again. They’re still strong now.”
Remy does have anaesthesia on his feet, and so is vulnerable to wounds. He’s had ulcers on his feet before and felt very ashamed and embarrassed because of this. “It’s another barrier to me getting a job.” He also has anaesthesia on his hands, so has to be particularly careful there too.
Two of his brothers, who don’t live here currently are also affected – one in Lukula, farming, and another in the nearby Angolan state of Cabinda.
TLM provided Remy and his father Fabien with beekeeping equipment, in particular the protective jacket, hat and gloves. There are 29 hives in total in the community. Fabien was trained by TLM in beekeeping in 2017. They sell the honey for $5 a litre. I bought a bottle and it is delicious – strong and earthy in flavour!
Thank you to TLM for contributing this story for #WorldLeprosyDay!

Joseph, 44, Lukula
Joseph is renting a tiny room from a landlady. We sit next door in her house as there’s space there.
His father is dead and his mother is mentally unwell. “I studied in school until class 2, but then dropped out when my father died.” Joseph was married, but when his wife found out he had leprosy she left him. He has three children. One of them, 16 is here with him. He was in school until class 3, but then left because the family lacked money. The kids all stopped school when Joseph got leprosy.
“I make money with difficulty. Friends sometimes help… this landlady has been good to me.”
Joseph’s hands and feet are quite badly affected by anaethesia, and manual work is difficult and tiring. Before he got leprosy he was a farm labourer.
“I got symptoms about 4 years ago. I was getting blisters on my hands. It wasn’t entirely painless. I went to see a traditional doctor who applied leaves to the various ulcers and wounds I had. I tried that for 3 years. My feet got worse in this time, and my nose collapsed too. I gave so much money to him. Before all of this I was a good farmer. But I’ve not been able to do anything. I’m starting to feel a bit better now.”
Joseph was eventually diagnosed and completed MDT 4 months ago.
“My wife likes money, and when I was earning we had a good relationship. But when I got sick, and got ulcers, I couldn’t work. There was no household conflict. She just left and went away. Apparently, she has remarried.”
His wife lives in Congo Brazzaville. He hasn’t seen her since she left. She has two of his kids with him. “I still speak to them by phone.” Joseph used to live there too, and came here to Lukula because he heard he may be able to get treated here.
“In the day I mainly just sleep at home, waiting for my wounds to heal. With my feet like this, what can I do? My landlady is a good woman. If I have money for rent I give it to her.”
Joseph’s younger brother is training his son to repair motorbikes.
“I feel very bad. It’s a hard life that I’m living. I didn’t go to school, and my children are also not going to school. I don’t have a job.”
Joseph does self-care.
I ask him what he hopes he could do. “I’d like to sell I think. Maybe have a shop. I have no feeling in my hands and feet, and I get cramps. I’m living with difficulty. If I have financial help I want to start a business selling food.”
Thank you to TLM for contributing this story for #WorldLeprosyDay!

Asi *, 15. Santé Centre Rural de Lukula
Asi * is here with her son who is 17 months. She’s still taking MDT for leprosy – 5 months out of 12 so far.
She completed class 6, but left in 2019 when she got pregnant. She lives with her mum Mbumbi and her little sister. Her father died when she was small.
In 2018 she saw patches on her face. She was spotted by a man doing active case-finding for leprosy in her area, a program initiated by TLM and the local health zone. The PLUBL project, funded by TLM Switzerland.
She was immediately put on MDT, and has had no other leprosy-related complications. She walks here once a month from Lumba. It takes her about 2 hours, and she carries her son the whole way.
Asi * now sells cassava leaves and wood and uses the income to take care of her child at home. “I get very sad. I have no husband, and it’s just me to take care of myself. My mum is worried and stressed all the time, and so I am too.”
“I just want to go back to school.” Asi * starts crying, while holding her son to her at the same time. It’s a deeply sad situation, that at least is no longer being exacerbated by leprosy.
“When I got it my mum was very worried. People used to tease me about my patches. When the community would all dress up on Sundays for church the ladies used to tease me about what skin lightening cream I was using.”
Asi ’s mother rents a house, but they struggle to pay the rent. “I was wondering if there was someone who could help me.” TLM is no longer doing income generating activities in the area sadly.
Asi ’s mother comes to the clinic shortly after the interview. She has concern etched onto her face. “The main problem is I… we want her to go back to school. But it’s difficult to pay the bills now too. So I sell peanuts.” Mbumbi makes around €0.40 profit per day. Rent is about €4.00 a month.
They are both very grateful leprosy is not a big problem in their life. Mbumbi says “I’m very thankful to the TLM staff and doctors who have helped diagnose my daughter, and provided the medicine free of charge.”
We realise it is likely a sensitive subject, but tentatively ask about her son. She doesn’t know where the father is. She used to see him on the way to and from school. They spoke quite a bit, and she knew he was an orphan. We don’t ask, and it’s difficult to tell how willing she was – of course being underage it’s not consensual. She gave birth by Caesarian aged 14. The father was 22 at the time.
Thank you to TLM for contributing this story for #WorldLeprosyDay!

Boishaki and her father
Boishaki is 13. Her father, Ram Babu, sat with us as we spoke to her. He was clearly worried about the impact of leprosy on her life. The family live in a very simple house – one big room with mud walls and corrugated metal roof, like most of the houses in the area.
She has one brother who is eight years old. Her mother and father also have leprosy – both are tea pickers
Boishaki has several white patches on her face. It started as only two patches but more keep appearing and as a young teenager she’s very conscious of this. She seemed uncomfortable at times and often looked down as we talked to her.
She was diagnosed with leprosy six months ago by TLM health workers who came to her home doing contact tracing of a known leprosy case in her community. Jiptha told us there are around 80 new cases in this very small area – leprosy is spreading fast.
She was very sad when she found out she had leprosy and she stopped going to school for a month as she wanted to hide the patches on her face. She is still trying to hide the fact she has leprosy from her school friends so she’s calling it a ‘skin disease’.
When asked how she feels she said she is scared she is getting more patches on her face and worried about what people will think.
She was diagnosed as a PB case and given MDT for 6 months but more patches are appearing – it’s likely thought that she is probably actually an MB case and if so she will need a longer course of Multidrug therapy. She has no other visible symptoms of leprosy.
She likes drawing and Bengali at school – said she might want to be an artist.
She also likes Kabadi and playing football. She supports some local Bangladeshi teams.
Her father worries that if people know she has leprosy she may not be able to go to school. She goes to a private school at the moment. The family live outside the tea gardens so there is stigma around leprosy in the community here [usually tea estates provide people with accommodation and within these communities there are low levels of stigma].
Both Boishaki and her father seemed very anxious about the future and the impact of leprosy on their family.